Recently talk show host Jimmy Fallon explained to his audience how a seemingly minor fall nearly cost him a finger – shedding light on a rare yet serious finger trauma known as a Ring Avulsion injury.
Ring avulsion results from the mechanism of crushing, shearing and avulsion, inducing severe macroscopic and microscopic damage. This type of injury often occurs when a ring that an individual is wearing is caught on an object, usually during a fall or jump. It can also occur when caught on fast moving equipment or just simply in a “freak” accident.
Damage from the abrupt and often harsh tug of the caught ring can range from a simple contusion to “degloving” of soft tissue – pulling the skin off circumferentially and stripping away the nerves, tendons and bone. Severe accidents may result in traumatic amputation of the finger.
Ring avulsion can be among one of the most devastating traumatic finger injuries, as often replantation following severe soft tissue damage is not possible – requiring revision amputation.
Fortunately, advances in microsurgery and interposition graft techniques have improved results with ring avulsion replantation. Patients should see a hand specialist immediately after the injury is identified.
Symptoms of Ring Avulsion
While Fallon knew he had severely injured his finger in his fall, the extent of the damage and seriousness of the injury was not completely revealed until his examination and x-ray. Prompt attention and surgical care from a specialized hand team fortunately saved his finger.
The severe damage that can occur in a ring avulsion case is not always evident to a patient. Immediate examination and x-ray assessment are necessary.
Symptoms may include:
- Pain
- Bleeding
- Lack of sensation at the tip
- Disfigurement
- Finger discoloration or whitening
In severe cases, part of the finger is removed from the bone or completely severed (traumatic amputation).
Diagnosing and Treating Ring Avulsion
When a patient presents with this type of finger trauma, the wound is cleaned and inspected for visible avulsed vessel, nerve, and tendon. Damaged skin edges are also assessed. An x-ray may also be indicated before determining the type of avulsion a patient has incurred. If a portion of the finger is separated, an x-ray is performed on both the amputated part and the remaining digit to fully asses damage and likelihood of replantation.
If there is a separated part, it is wrapped in a saline gauze and placed in a bag with ice water. The patient is given antibiotics and tetanus prophylaxis.
The injury is then classified using one of several ring avulsion classification systems that exist. Most commonly used is the Urbaniak Classification system. The class of ring avulsion (Class 1, 2, or 3) will help determine treatment.
The goal of the hand surgeon is to salvage, maintain function and, if possible, provide an esthetic appearance.
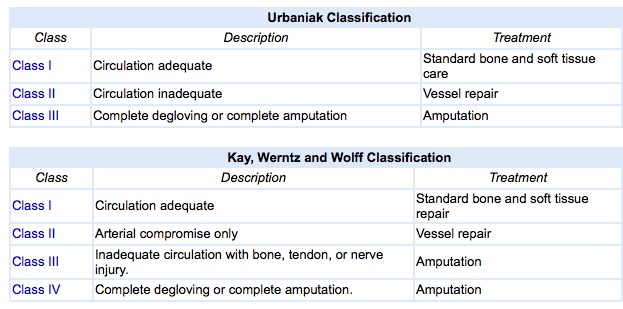
Commonly used classification charts for Ring Avulsion injuries.
Avoiding Risk of Ring Avulsion
It is difficult for patients to understand how otherwise inconsequential stumbles or movements can result in the damage or loss of a digit when a ring is involved. We often forget that the bones and joints of the hand and wrist are small and capable of sustaining just so much force. Skin is the finger’s strongest part. Once the skin tears, the remaining tissue quickly degloves. Though rare, the potential harm that a ring can pose should be considered – particularly when performing certain extracurricular or sports activities, or when working with machinery. Unfortunately many accidents resulting in a ring avulsion are not anticipated nor could be imagined. Prompt attention is key to a successful outcome.
References
Flagg SV, Finseth FJ, Krizek TJ. Ring avulsion injury. Plast Reconstr Surg. 1977;59:241–8.
Brooks D, et al. Ring avulsion: injury pattern, treatment, and outcome. Clinics in Plastic Surgery April 2007 ;34(2):187-95, viii.
Fejjal N, Belmir R, Mazouz S El, Gharib NE, et al. Finger avulsion injuries: A report of four cases. Indian J Orthop. 2008 Apr-Jun; 42(2): 208–211.
Sears ED, Chung KC. Replantation of finger avulsion injuries: A systematic review of survival and functional outcomes. J Hand Surg Am. 2011;36(4):686-94.
Comments are closed.