Hand and upper extremity injuries account for over half of the orthopedic injuries seen in an ER or Urgent care center.

Fractures among most common ER/Urgent Care injuries
According to a 2012 study published in the Hand journal, the most common region injured is the finger (38.4%), and the most common upper extremity injury was a fracture (29.2%). Specific injuries with high incidence rates (all per 100,000 per year) included finger lacerations (221), wrist fractures (72), finger fractures (68), and lower arm fractures (64). [1]
While home is cited as the most common setting for an upper extremity injury, sports injuries in the field run a close second.
A few of the most common hand and upper extremity injuries include:
- Contusions and Lacerations
- Fractures
- Sprains and Dislocations
Hand and Upper Extremity Contusions and Lacerations
Contusions and lacerations can result from an accident, fall or sports injury. Both should be carefully assessed, as damage to nerves, tendons and bone may exist.
Contusions
Contusions occur when a direct blow strikes part of the body, crushing underlying muscle fibers and connective tissue without breaking the skin.
Contusions cause swelling and pain, and limit joint range of motion near the injury. Torn blood vessels may cause bluish discoloration (bruising). The injured muscle may feel weak and stiff.
Sometimes a pool of blood collects within damaged tissue, forming a lump over the injury known as a hematoma. Swelling and bleeding beneath the skin in severe cases may cause shock. If tissue damage is extensive, there may also be a broken bone, dislocated joint, sprain, torn muscle, or other injury.
Diagnostic tools used to assess the extent of the damage may include ultrasound, magnetic resonance imaging (MRI), or computed tomography (CT) scans. For some injuries, testing for nerve injury may also be indicated. Treatment will depend on the extent of the injury, though RICE (Rest, Ice, Compression, Elevation) is encouraged for contusions until a physician can be seen.
Follow up is important to thoroughly assess the scope of soft tissue damage. Complications that can occur from contusions include compartment syndrome and myositis ossificans.
Lacerations
Lacerations often result from a cut with a knife, piece of glass or other sharp object. It can be difficult for patients to determine how deep and how damaging a laceration may be.
Concerns include:
- Length and depth of cut (more than 1/4” deep with visible deep tissue)
- Visible bone
- Width of cut and inability to squeeze skin closed
- Severe bleeding
- Cleanliness of cut (item causing cut) and possible debris in the wound
An ER or Urgent Care clinic can address these types of injuries, properly cleaning the wound and bandaging and/or suturing (stitching). Lacerations of the hand and upper extremity should be further evaluated by a specialist to determine if there is damage to surrounding nerves, tendons or other soft tissue. If unaddressed permanent loss of sensation or range of motion can result.
Hand and Upper Extremity Sprains and Dislocations
Unlike a fracture, sprains and dislocations do not cause a break in the bone. These types of injuries are usually the result of extreme stretching of the limb, occurring from a twist, hit or fall. A sprain is a tear (minor or severe) in a ligament, which connects bones. Symptoms may include pain, swelling, and bruising.
A dislocation occurs when the bones meeting at a joint are disrupted and moved out of their natural alignment. This is a common injury to the fingers. Symptoms may include severe pain during movement and an obvious deformity.
While initial treatment will depend on the severity of the injury, most sprains will resolve on their own with RICE (rest, ice, compression and possibly elevation). A dislocation may require reduction (placing the joint back into proper alignment) and a brief period of immobilization with a splint. Injuries should be assessed more thoroughly by a specialist to ensure that there is no further damage to surrounding nerves, ligaments or tendons.
Hand and Upper Extremity Fractures
Fractures are among the most commonly seen injuries in the ER or Urgent Care setting.
Fracture type can vary and are treated differently in the adolescent child and adult.
These types of injuries most commonly occur to the shoulder, elbow, wrist, and hand/finger as a result of a fall onto an outstretched arm or block from a harsh impact. This is particularly true of sports injuries.
With both the frequency and intensity of youth sports participation higher than ever, understanding the significant anatomical differences between the skeletally immature patient and the skeletally mature patient is also key in properly identifying and treating the variety of musculoskeletal injuries that occur to the hand and upper extremity.
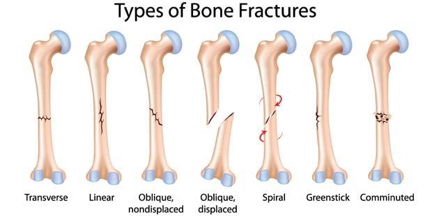
Fracture Type
There are many different types of fractures, all of which fall into one of two categories – displaced and non displaced. A displaced fracture means that the parts of the bone at the break are not in alignment and require realignment before healing can begin. A non displaced fracture means that the break did not disrupt the alignment of the bone.
A displaced fracture can sometimes cause the bone to pierce through the skin, which is known as an open or compound fracture.
Because the lining of the bone is thicker in children, diminishing with age, the most common fractures seen in adolescents are non displaced buckle and greenstick fractures (affecting the wrist and forearm bones). In adults, fractures tend to be more severe – often displaced and comminuted (multiple bone fragments requiring more complicated reassembly). Common fractures seen in adults are wrist fractures (distal radius fractures and scaphoid fractures).
An x-ray will help determine the type of fracture and best treatment. Initially, most fractures can be safely splinted and supported with a sling, until an orthopedic specialist is seen. Prompt followup with an orthopedic physician is important, particularly for displaced fractures. Most ER and Urgent Care centers will provide patients with a digital copy of their x-ray for followup with a specialist.
Fracture Care
Most non displaced fractures heal well with a period of casting followed by rehabilitation exercises. Displaced fractures first require realignment, which is known as either closed reduction (non surgical) or open reduction (surgical). Surgical repair will also include internal fixation with plates and screws to ensure the bone pieces remain aligned while healing.
Close followup with a hand and upper extremity specialist is key for proper healing of fractures and reduced risk of future problems affecting the injured bone and nearby joints.
References
1.) Daan Ootes, Kaj T Lambers, David C Ring. The epidemiology of upper extremity injuries presenting to the emergency department in the United States. Hand (NY). 2012;7(1):18-22. Published online 2011 Dec 14. doi: 10.1007/s11552-011-9383-z
Comments are closed.